Like any other criminal mob every aspect of the American health care industry AKA the Medical Mafia is corrupt and inept. They could fuck up a one man parade.
Abstract
While many areas of health care are still struggling with the issue of patient safety, laboratory diagnostics has always been a forerunner in pursuing this issue. Significant progress has been made since the release of “To Err is Human.”1 This article briefly reviews laboratory quality assessment and looks at recent statistics concerning laboratory errors.
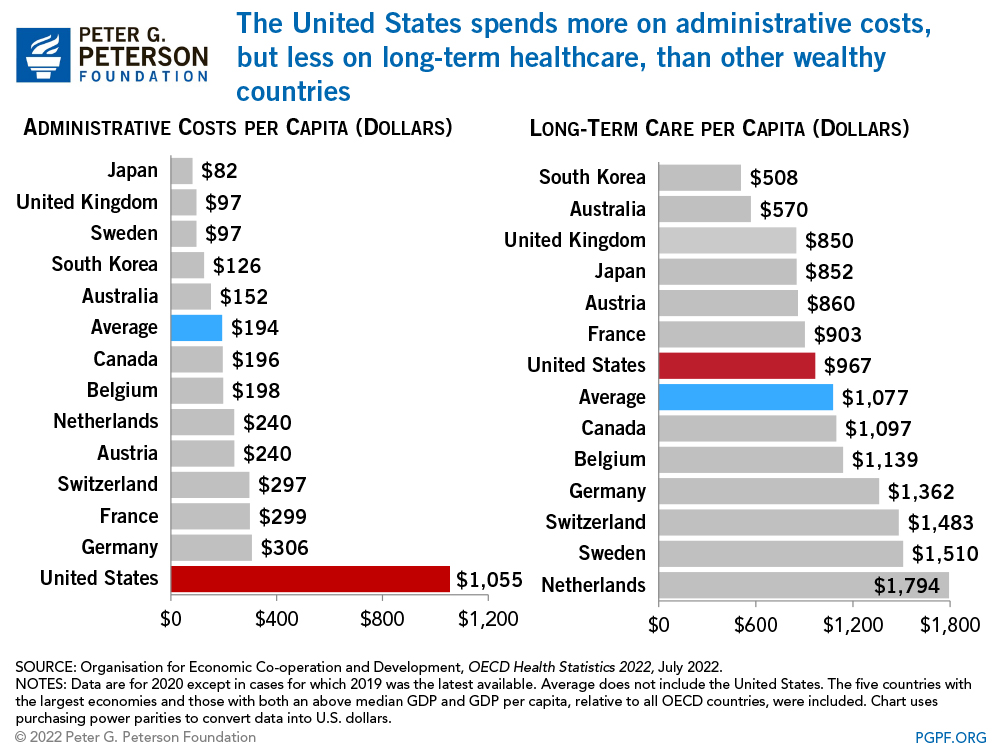
It has been 12 years since the Institute of Medicine (IOM) reported the alarming data on the cause and impact of medical errors in the United States.1 Besides causing serious harm to patients, medical errors translate into huge costs for the national economy. In 1999, Berwick and Leape published that the estimated cost of medical errors in the United States was between $17 billion-$29 billion a year.2 In 2006, Null and colleagues published an article indicating the overall estimated annual economic cost of improper medical intervention was much higher, approaching $282 billion.3 While many areas of health care are still struggling with the issue of patient safety, laboratory diagnostics has always been a forerunner in pursuing this issue. The concepts and practices of quality assessment programs have long been routine in laboratory medicine, and error rates in laboratory activities are far lower than those seen in overall clinical health care.4 This article briefly reviews laboratory quality assessment and looks at recent statistics concerning laboratory errors.
Quality Standards
Laboratory medicine sets high quality standards. Regulation of quality in the health care sector is based on accreditation, certification, quality monitoring, patient’s rights, standard operation processes, and standards of health care quality.5 The Centers for Medicare and Medicaid Services (CMS) regulates all laboratory testing (except research) performed on humans in the United States through the Clinical Laboratory Improvement Amendments (CLIA). The Division of Laboratory Services, within the Survey and Certification Group, under the Center for Medicaid and State Operations (CMSO), has the responsibility for implementing the CLIA program. The objective of the CLIA program is to ensure quality laboratory testing.6
In order for a health care organization to participate in and receive payment from Medicare or Medicaid programs, it must be certified as complying with the Conditions of Participation (CoP), or standards, set forth in federal regulations. This certification is based on a survey conducted by a state agency on behalf of CMS. However, if a national accrediting organization, such as The Joint Commission (TJC), formerly known as the Joint Commission on Accreditation of Health Care Organizations, has and enforces standards meeting the federal CoP, CMS may grant the accrediting organization “deeming” authority and “deem” each accredited health care organization as meeting the Medicare and Medicaid certification requirements. The health care organization is then considered to have “deemed status” and is not subject to the Medicare survey and certification process. Laboratories can also be accredited by the College of American Pathologists (CAP) and the Commission on Office Laboratory Accreditation (COLA), both of which also have deemed status with CMS.7,8,9
Sources of Laboratory Error
Traditionally, laboratory practice can be divided into 3 phases (pre-analytical, analytical, and post-analytical). All 3 phases of the total testing process can be targeted individually for improving quality, although it is well published that most errors occur in the pre- and post-analytical phases (Table 1).10 In the field of laboratory medicine, Lippi and colleagues published that the total testing process error rate ranges widely from 0.1% to 3.0%.11 In studies done by Plebani and Carraro, laboratory error rates declined over 10 years from 0.47% in 1977 to 0.33% in 2007.12,13 A similar declining trend has been seen specifically in analytical errors. The analytical variability is now frequently less than 1/20th of what it was 40 years ago.14 Analytical mistakes now count for <10% of all mistakes.12
Analytical Error
Focusing first on the analytical phase of laboratory testing, the analytical phase begins when the patient specimen is prepared in the laboratory for testing, and it ends when the test result is interpreted and verified by the technologist in the laboratory. Not processing a specimen properly prior to analysis or substances interfering with assay performance can affect test results in the analytical phase. Establishing and verifying test method performance specifications as to test accuracy, precision, sensitivity, specificity, and linearity are other areas where errors can occur in the analytical phase of laboratory testing.
The laboratory has spent decades improving analytical quality by establishing internal quality controls (IQC) and external quality assessment (EQA). The role of EQA and proficiency testing (PT) is to provide reliable information allowing laboratories to assess and monitor the quality status of internal procedures and processes, the suitability of the diagnostic systems, the accountability and competence of the staff, along with the definition of measurement uncertainty in laboratory results. The responsibility of laboratory professionals is to appropriately analyze EQA/PT samples and reports, detect trends or bias that may not be apparent in single results, investigate root causes producing unacceptable performances, apply and monitor opportune actions for removing the underlying cause(s), verify the effectiveness, and, above all, determine whether the problem affected clinical decision making.15
Pre-analytical Error
The pre-analytical phase of the total laboratory testing process is where the majority of laboratory errors occur. Pre-analytical errors can occur at the time of patient assessment, test order entry, request completion, patient identification, specimen collection, specimen transport, or specimen receipt in the laboratory. A report by Bonini and colleagues found that pre-analytical errors predominated in the laboratory, ranging from 31.6% to 75%.16 In 2008 to 2009, Chawla and colleagues performed a 1-year study in the clinical chemistry laboratory on the frequency of pre-analytical errors observed in both inpatients and outpatients. For the inpatients, a pre-analytical error rate of 1.9% was reported. The variable receiving the highest frequency rating was specimen hemolysis at 1.10%. For the outpatients, the error rate was 1.2%, and the variable with the highest frequency rating was insufficient volume for testing.17 Some of the other common sources of pre-analytical error are the following: ordering tests on the wrong patient, ordering the wrong test, misidentifying the patient, choosing the inappropriate collection container, or labeling containers improperly.
A comprehensive plan to prevent pre-analytical errors has 5 interrelated steps:
Developing clear written procedures.
Enhancing health care professional training.
Automating functions, both for support operations and for executive operations.
Monitoring quality indicators.
Improving communication among health care professionals and fostering interdepartmental cooperation.18,19,20
| Phase of Total Testing Process | Type of Error | Rates |
|---|---|---|
| Pre-analytical | Inappropriate test request | 46%–68.2% |
| Order entry errors | ||
| Misidentification of patient | ||
| Container inappropriate | ||
| Sample collection and transport inadequate | ||
| Inadequate sample/anticoagulant volume ratio | ||
| Insufficient sample volume | ||
| Sorting and routing errors | ||
| Labeling errors | ||
| Analytical | Equipment malfunction | 7%–13% |
| Sample mix-ups/interference | ||
| Undetected failure in quality control | ||
| Procedure not followed | ||
| Post-analytical | Failure in reporting | 18.5%–47% |
| Erroneous validation of analytical data | ||
| Improper data entry |
Written procedures must clearly explain how to identify a patient, collect and label a specimen, and subsequently transport the specimen and prepare it for analysis. Those individuals performing the pre-analytical procedures must understand not only what the procedures are but why they are important to follow. They need to know not only what happens if the correct steps are not followed, but also what errors can occur and what effect they can have on the sample and ultimately the patient. There must be ongoing training for these employees and competencies must be assessed annually.21
Modern robotic technologies and information systems can also help reduce pre-analytical errors. Computerized order entry simplifies test ordering and eliminates a second person from transcribing the orders. Automated phlebotomy tray preparation provides a complete set of labeled blood tubes and labels for hand labeling in a single tray for each patient. Pre-analytical robotic workstations automate some of the steps and reduce the number of manual steps involving more people. Barcodes also simplify specimen routing and tracking.21
Recent advances in laboratory technology have made available new and more reliable means for the automated detection of the serum indices, including the hemolysis index. Visual detection of hemolysis must be abandoned due to low sensitivity and low reproducibility. Laboratory personnel must ask for new samples when hemolysis is detected. If a new sample cannot be obtained, it is the responsibility of the laboratory specialist to communicate the problem to the clinician. The data obtained from the serum indices can be used to monitor the quality of the collection process.22
Post-analytical Error
In the post-analytical phase of the testing process, results are released to the clinician, and s/he interprets them and makes diagnostic and therapeutic decisions accordingly. Such things as inappropriate use of laboratory test results, critical result reporting, and transmission of correct results are areas of potential error in the post-analytical phase of the total laboratory testing process.
In an article by Plebani and Piva, the authors give a comprehensive overview on the ongoing efforts for improving actual consensus on the definition and notification of laboratory critical values, and for evaluating their contribution to improve clinical outcomes and patient safety. The article also provides some highlights on a valuable experience of automated notification, which is a reliable tool for improving the timeliness of communication and avoiding potential errors for which accreditation programs require read-back of the results.23
Monitoring Errors
The success of any efforts made to reduce errors must be monitored in order to assess the efficacy of the measures taken. Quality indicators must be used for assessment. In the testing process areas involving non-laboratory personnel, interdepartmental communication and cooperation are crucial to avoid errors. Therefore the entire health care system must be involved in improving the total testing process. There must be adequate and effective training of personnel throughout the institution to be competent in following processes and procedures.21
Incident Reporting in Laboratory Diagnostics
While major efforts have been made to monitor the pre-analytical phase and provide reliable solutions, it is surprising that concrete formal programs of incident reporting have not been so pervasive in laboratory diagnostics.24 The major focus in health care is placed on incident reporting for several medical conditions with lesser effort devoted to translating this noteworthy practice into laboratory diagnostics. If, in fact, laboratory errors are being underreported, then current statistics reveal only a small portion of the medical errors actually taking place. There is an urgent need to establish a reliable policy of error recording, possibly through informatics aids,25 and settle universally agreed “laboratory sentinel events” throughout the total testing process, which would allow gaining important information about serious incidents and holding both providers and stakeholders accountable for patient safety. Some of these sentinel events have already been identified, including inappropriate test requests and patient misidentification (pre-analytical phase), use of wrong assays, severe analytical errors, tests performed on unsuitable samples, release of lab results in spite of poor quality controls (analytical phase), and failure to alert critical values and wrong report destination (post-analytical phase).26,27 The Drafting Group of WHO’s International Classification for Patient Safety (ICPS) has also developed a conceptual framework that might also be suitable for diagnostics errors.28
Development and widespread implementation of a Total Quality Management (TQM) system is the most effective strategy to minimize uncertainty in laboratory diagnostics. Pragmatically, this can be achieved using 3 complementary actions: preventing adverse events (error prevention), making them visible (error detection), and mitigating their adverse consequences when they occur (error management).24
Other methodologies can also be used to prevent errors. Failure Mode and Effect Analysis (FMEA) has been a broadly cited reliable approach to risk management. It is a systematic process for identifying potential process failures before they occur, with the aim to eliminate them or minimize the relative risk. The U.S. Department of Veteran Affairs National Center for Patient Safety developed a simplified version of FMEA to apply to health care, called Healthcare FMEA (HFMEA).29 Root Cause Analysis (RCA) is an additional valuable aid, since it is based on a retrospective analytical approach. A RCA focuses on identifying the latent conditions underlying variation in medical performance and, if applicable, developing recommendations for improvements to decrease the likelihood of a similar incident in the future.11
Conclusion
Patient safety emphasizes the reporting, analysis, and prevention of medical errors that often lead to adverse events. Besides carrying serious harms to patient health, medical errors translate into a huge amount of money wiped out of the national and international economy. Significant progress has been made since the release of “To Err is Human.” Basically what has changed is the willingness to recognize the challenge and not argue about the numbers, but appreciate care must be safe always and everywhere for each patient. This has led to remarkable changes in the culture of health care organizations, so medical errors can no longer be seen as inevitable, but as something that can be actively streamlined and prevented.24