American Spine Surgeons are the worst in the industrialized world as well as highest paid and greediest. That may be why most of them don't recommend traction for disk hernias.
The following study was conducted in Korea so chances are it is more reliable and honest than anything you will find in the greedy US.
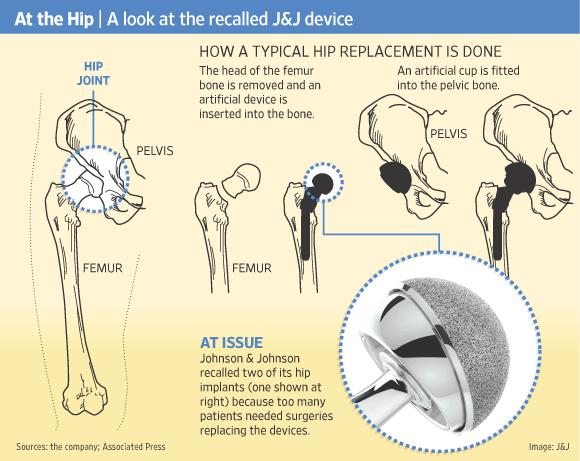
Reducibility of Cervical Disk Herniation: Evaluation at MR Imaging during Cervical Traction with a Nonmagnetic Traction Device
- Tae-Sub Chung, MD,
- Young-Jun Lee, MD,
- Seong-Woong Kang, MD,
- Chang-Jun Park, MD,
- Won-Suk Kang, MSc and
- Yong-Woon Shim, MD
-
1From
the Department of Diagnostic Radiology and Research Institute of
Radiological Science, Brain Korea 21 Project for Medical
Science (T.S.C., Y.J.L., W.S.K., Y.W.S.), and
Department of Rehabilitation Medicine (S.W.K.), Yonsei University
College of
Medicine, YongDong Severance Hospital, 146-92
Dogok-Dong, Kangnam-Gu, Seoul 135-270, Korea; and Airtrac MSI, Seoul,
Korea
(C.J.P.). From the 2000 RSNA scientific
assembly. Received July 17, 2001; revision requested September 17; final
revision
received March 25, 2002; accepted May 14.
Supported by Airtrac grant 1999-31A1-00014. Address correspondence to T.S.C. (e-mail: tschung@yumc.yonsei.ac.kr).
Abstract
The authors evaluated the reducibility of
cervical disk herniation at magnetic resonance (MR) imaging performed
with the patient
in cervical traction. After the acquisition of
neutral-state images, cervical traction images were obtained in 29
patients
and seven healthy volunteers while they wore a
portable intermittent traction device. During traction, all volunteers
and
21 patients had a substantial increase in the
length of the cervical vertebral column. The disk herniation was
completely
resolved in three patients and partially reduced in
18. The reducibility of cervical disk herniation can be evaluated at MR
imaging performed during cervical traction.
Cervical traction has been applied widely to relieve neck pain from muscle spasm or nerve compression in rehabilitation medicine
settings (
1,
2). Continuous or intermittent traction has been regarded as an effective treatment for herniated cervical disks (HCDs) because
it facilitates widening of the disk spaces (
3,
4). The traction induces pain relief and regression of the herniated disks. Several reports (
5–
7) have described the regression of herniated disks either spontaneously or within the treatment period.
Widening of disk space during traction has been demonstrated mostly on radiographs (
1).
Radiography does not yield direct images of the herniated disk,
however; radiographs show only the changes in vertebral
bone structures. Direct visualization of the cervical
disk would be very helpful for evaluating the reducibility of disk
herniation
during traction, and magnetic resonance (MR) imaging
is the best examination for evaluation of intervertebral disk problems.
To our knowledge, however, a device that enables
visualization of the cervical disk during traction and is applicable to
MR
imaging has not been available before now. Although a
portable traction device for cervical fractures has been reported on,
the report was in the form of a technical note
regarding a portable traction device that can be used with myelography
or computed
tomography (CT) (
8).
The study was not applicable to MR imaging because the metallic
composition of the described traction device produced substantial
artifacts.
We have designed a portable intermittent
traction device made of nonmagnetic materials that do not affect MR
imaging. The
purpose of our study was to evaluate the reducibility
of cervical disk herniation at MR imaging performed with the patient
in cervical traction.
Materials and Methods
For 19 months, from June 1999 to November
2000, a total of 29 patients who consecutively received a diagnosis of
HCD on the
basis of findings at previously performed cervical
CT or MR imaging and seven healthy volunteers were examined at cervical
spinal MR imaging. The healthy volunteers were
selected from a group of young persons during two stages: First, a
rehabilitation
physician (S.W.K.) selected young (ie, aged 18–40
years) healthy volunteers if they had none of the following symptoms or
signs: pain, stiffness, tenderness, fracture,
dislocation, neurologic signs such as decreased or absent deep tendon
reflexes,
weakness, sensory deficits, or muscular signs such
as decreased range of motion or point tenderness. Next, the selected
volunteers
underwent T2-weighted MR imaging while in a neutral
(ie, nontraction) state, and if either a degenerative change in or a
herniation
of a disk was detected, the subject was excluded.
Finally, the selected volunteers underwent MR imaging while wearing the
inflated traction device.
The patient group consisted of 10 men and
19 women, who ranged in age from 25 to 62 years (mean age, 44.4 years).
The healthy
volunteer group consisted of one man and six women,
who ranged in age from 19 to 37 years (mean age, 26 years). The MR
imaging
examinations were performed after informed consent
had been obtained from all patients and volunteers, as was required by
the institutional review board of Yonsei University
College of Medicine, YongDong Severance Hospital.
Traction Device
The traction device (
Fig 1)
was originally designed for portable intermittent use to accommodate a
patient’s daily activities during traction. It is
also constructed of a nonmagnetic material
(Airtrac 101; Airtrac MSI, Seoul, Korea) that is compatible to MR
imaging units.
The traction device consists of three main
parts:
(a) a shoulder cover for the base of the device,
(b) an accordion-shaped middle component that can be expanded by means of air inflation, and
(c)
mandible supports for effective transmission of traction. When the
device is inflated with air, the accordion-shaped middle
component stretches and has a traction effect on
the neck. The anterior portion of the middle component is fixed with a
band
to maintain a flexion posture of the neck. We
used 30 pounds of traction force: The pressure to the internal space was
0.4
kgf/cm
2. Immediately after the procedure, we asked the volunteers and patients if they had experienced any pain or other discomfort
during inflation of the traction device or during imaging.
Figure 1a. Cervical traction device used on a healthy volunteer. (a, b) The traction device consists of a shoulder cover at the base of the device (1), an accordion-shaped middle component that is expanded by means of air inflation (2), and mandible supports for effective transmission of traction (3). In b, the anterior portion (4) of the middle component is fixed with a band to maintain a flexion posture of the neck. (c, d) When the device is inflated with air, the accordion-shaped middle component stretches to have a traction effect on the neck.
Figure 1b. Cervical traction device used on a healthy volunteer. (a, b) The traction device consists of a shoulder cover at the base of the device (1), an accordion-shaped middle component that is expanded by means of air inflation (2), and mandible supports for effective transmission of traction (3). In b, the anterior portion (4) of the middle component is fixed with a band to maintain a flexion posture of the neck. (c, d) When the device is inflated with air, the accordion-shaped middle component stretches to have a traction effect on the neck.
Figure 1c. Cervical traction device used on a healthy volunteer. (a, b) The traction device consists of a shoulder cover at the base of the device (1), an accordion-shaped middle component that is expanded by means of air inflation (2), and mandible supports for effective transmission of traction (3). In b, the anterior portion (4) of the middle component is fixed with a band to maintain a flexion posture of the neck. (c, d) When the device is inflated with air, the accordion-shaped middle component stretches to have a traction effect on the neck.
Figure 1d. Cervical traction device used on a healthy volunteer. (a, b) The traction device consists of a shoulder cover at the base of the device (1), an accordion-shaped middle component that is expanded by means of air inflation (2), and mandible supports for effective transmission of traction (3). In b, the anterior portion (4) of the middle component is fixed with a band to maintain a flexion posture of the neck. (c, d) When the device is inflated with air, the accordion-shaped middle component stretches to have a traction effect on the neck.
MR Imaging
All MR imaging studies were performed
by using a 1.5-T MR system (Vision; Siemens, Erlangen, Germany) with
25-mT/m gradient
capability. With the patient wearing the
traction device, standard cervical spinal MR images were acquired with
sagittal turbo
spin-echo T2-weighted and transverse
two-dimensional fast low-angle shot sequences by using a standard spine
circular polarization
array coil. The parameters for sagittal turbo
spin-echo T2-weighted MR imaging were 4,000/128 (repetition time
msec/echo time
msec), a 138 × 256 matrix, a 156 × 250-mm field
of view, and nine images of 3-mm section thickness obtained during an
acquisition
time of 52 seconds. The parameters for
transverse two-dimensional fast low-angle shot MR imaging were 550/12, a
30° flip angle,
a 112 × 256 matrix, a 125 × 200-mm field of
view, and nine images of 3-mm section thickness obtained during an
acquisition
time of 2 minutes 5 seconds. We reduced the
matrix number to less than that used to obtain standard MR images, to
minimize
the acquisition time and motion artifacts.
First, neutral-state images were
obtained during deflation of the traction device. Then, traction-state
images were obtained
10 minutes after inflation with an external air
tube to allow time for the traction effect on the normal or herniated
disk.
The patients and volunteers were monitored with
closed-circuit television surveillance and could communicate by means of
microphone
to prevent unexpected emergency situations
during traction.
Image Analysis
As a parameter of cervical vertebral
column elongation, the distance between the middle point of the superior
border of the
C1 anterior arch and the inferoposterior point
of the C7 vertebral body on magnified sagittal MR images was measured by
using
the computer console of the MR imaging unit
(Vision). We did not use the odontoid process as the superior landmark
because
exact localization of the odontoid process tip
could have been difficult sometimes owing to a patient’s tilting or
rapid position
change during traction. Measurements of cervical
vertebral column elongation were obtained by two neuroradiologists
(T.S.C.,
Y.J.L.) separately and blindly. The
neuroradiologists were not informed of the patients’ clinical
information.
The reducibility of cervical disk
herniation was evaluated in the patient group. Complete resolution of
the herniation was
defined as a result in which the disk was
completely inside the annulus margin without a residual herniated disk
particle.
Partial reduction was defined as a more than 50%
volume reduction in the herniated disk particle with some residual
tissue.
The reduction ratio was calculated as follows:
[(
D −
d)/
D] × 100, where
D is the distance between two parallel lines—one line drawn at the base of the herniated disk particle and the other drawn
at the tip—in the neutral state and
d is this distance in the traction state (
Fig 2).
Figure 2. Measurement of reduction ratio. Reduction ratio was calculated as follows: [(D − d)/D] × 100. D is the distance between two parallel lines—one line drawn at the base of the herniated disk particle and the other drawn
at the tip—in the neutral state, and d is this distance in the traction state.
Whether there was widening of the
facet joints or intervertebral foramen during traction was determined in
the patients and
healthy volunteers. Retraction of the posterior
margin of the disk during traction, as depicted on sagittal MR images,
also
was evaluated in the volunteers and patients. If
the retracted posterior margin of the disk passed an imaginary line
drawn
from the posterior margins of two adjacent
vertebral bodies, we defined this phenomenon as dimpling.
The two radiologists evaluated the
pre- and post traction images side by side, without knowledge of the
patients’ clinical
information. The radiologists reviewed the
images simultaneously, and results were recorded when they reached a
consensus.
Statistical Analysis
The extent of cervical vertebral
column elongation in the patients during traction was compared with that
in the healthy volunteers.
Statistical analysis was performed by using
computer software (SPSS; SPSS, Chicago, Ill and Excel 2000; Microsoft
Korea, Seoul,
Korea). The Mann-Whitney U test was used to analyze our study data, and a P value of less than .05 was considered to indicate a statistically significant difference.
Results
The MR images obtained in the seven
healthy volunteers during traction showed that the length of the
cervical vertebral column
had increased by 0–3 mm (mean length increase, 1.93
mm). Of the 29 patients, 21 (72%) had complete resolution or partial
reduction
of the cervical disk herniation and an elongation
of the cervical vertebral column of 0–7 mm (mean length increase, 2.19
mm),
which was not significantly different from that in
the volunteers (
P = .917). Eight patients had minimal elongation of the cervical vertebral column (mean length increase, 0.44 mm), which was
significantly shorter than that in the healthy volunteers (
P < .001) (
Table 1). No patient reported having pain or any other discomfort during either traction device inflation or MR imaging.
TABLE 1. Increased Length of Cervical Vertebral Column during Traction
Of the 29 patients, who had a total of 40
HCDs, 19 had an HCD at one cervical disk level, nine had HCDs at two
levels, and
one had HCDs at three levels. There were 15 HCDs
each at the C5–6 and C6-7 cervical disk levels. There were five HCDs at
the
C3-4 level, three at the C4-5 level, and two at the
C7-T1 level. In the patient with HCDs at three levels, the herniation
at one level was reduced but the herniations at the
two remaining levels were not. In the nine patients with HCDs at two
levels
(total of 18 levels), the herniations were reduced
at 13 levels and not reduced at five levels. Of the 19 patients with
HCDs
at one level, 13 had reduced herniations and six
did not.
Disk herniation was completely resolved in three (10%) of the 29 patients (
Fig 3) and partially reduced in 18 (62%) (
Fig 4).
Eight of the 29 patients had minimal elongation of the cervical
vertebral column during traction (mean length increase,
0.44 mm; range, 0–1.5 mm), however, and no
reduction of the disk herniation. The length of elongation of the
cervical vertebral
column during traction in this group was
significantly shorter than that in the healthy volunteers (
P = .02). There was a significant difference in elongation of the vertebral column between the patients who did and those who
did not have some herniation reduction (
P = .01).
Figure 3a.(a, b) Sagittal (4,000/128) and (c, d) transverse
(two-dimensional fast low-angle shot sequence, 550/12, 30° flip angle)
MR images depict a completely resolved cervical
disk herniation after traction. (a, c) Neutral-state MR images show extrinsic compression of the dural sac and spinal cord at the C5-6 cervical disk level due to
an HCD (arrow). (b, d) Traction-state MR images show reduction of the cervical disk herniation and the residual deformed spinal cord. Widening of
the right-side facet joint space (arrow in d) is seen on the transverse traction-state image.
Figure 3b.(a, b) Sagittal (4,000/128) and (c, d) transverse
(two-dimensional fast low-angle shot sequence, 550/12, 30° flip angle)
MR images depict a completely resolved cervical
disk herniation after traction. (a, c) Neutral-state MR images show extrinsic compression of the dural sac and spinal cord at the C5-6 cervical disk level due to
an HCD (arrow). (b, d) Traction-state MR images show reduction of the cervical disk herniation and the residual deformed spinal cord. Widening of
the right-side facet joint space (arrow in d) is seen on the transverse traction-state image.
Figure 3c.(a, b) Sagittal (4,000/128) and (c, d) transverse
(two-dimensional fast low-angle shot sequence, 550/12, 30° flip angle)
MR images depict a completely resolved cervical
disk herniation after traction. (a, c) Neutral-state MR images show extrinsic compression of the dural sac and spinal cord at the C5-6 cervical disk level due to
an HCD (arrow). (b, d) Traction-state MR images show reduction of the cervical disk herniation and the residual deformed spinal cord. Widening of
the right-side facet joint space (arrow in d) is seen on the transverse traction-state image.
Figure 3d.(a, b) Sagittal (4,000/128) and (c, d) transverse
(two-dimensional fast low-angle shot sequence, 550/12, 30° flip angle)
MR images depict a completely resolved cervical
disk herniation after traction. (a, c) Neutral-state MR images show extrinsic compression of the dural sac and spinal cord at the C5-6 cervical disk level due to
an HCD (arrow). (b, d) Traction-state MR images show reduction of the cervical disk herniation and the residual deformed spinal cord. Widening of
the right-side facet joint space (arrow in d) is seen on the transverse traction-state image.
Figure 4a.(a, b) Sagittal (4,000/128) and (c, d) transverse (two-dimensional fast low-angle shot sequence, 550/12, 30° flip angle) MR images of a partially reduced cervical
disk herniation after traction. (a, c) Neutral-state MR images show a small area of high signal intensity (arrow) that corresponds to a herniated disk fragment in
the posterior central direction at the C5-6 cervical disk level. (b, d) Traction-state MR images show a reduction of the fragment (arrow in b) through a torn tract of the annulus fibrosus at the C5-6 cervical disk level.
Figure 4b.(a, b) Sagittal (4,000/128) and (c, d) transverse (two-dimensional fast low-angle shot sequence, 550/12, 30° flip angle) MR images of a partially reduced cervical
disk herniation after traction. (a, c) Neutral-state MR images show a small area of high signal intensity (arrow) that corresponds to a herniated disk fragment in
the posterior central direction at the C5-6 cervical disk level. (b, d) Traction-state MR images show a reduction of the fragment (arrow in b) through a torn tract of the annulus fibrosus at the C5-6 cervical disk level.
Figure 4c.(a, b) Sagittal (4,000/128) and (c, d) transverse (two-dimensional fast low-angle shot sequence, 550/12, 30° flip angle) MR images of a partially reduced cervical
disk herniation after traction. (a, c) Neutral-state MR images show a small area of high signal intensity (arrow) that corresponds to a herniated disk fragment in
the posterior central direction at the C5-6 cervical disk level. (b, d) Traction-state MR images show a reduction of the fragment (arrow in b) through a torn tract of the annulus fibrosus at the C5-6 cervical disk level.
Figure 4d.(a, b) Sagittal (4,000/128) and (c, d) transverse (two-dimensional fast low-angle shot sequence, 550/12, 30° flip angle) MR images of a partially reduced cervical
disk herniation after traction. (a, c) Neutral-state MR images show a small area of high signal intensity (arrow) that corresponds to a herniated disk fragment in
the posterior central direction at the C5-6 cervical disk level. (b, d) Traction-state MR images show a reduction of the fragment (arrow in b) through a torn tract of the annulus fibrosus at the C5-6 cervical disk level.
Widening of the facet joint space was observed at MR imaging during traction in two (29%) of the seven healthy volunteers
and in five (17%) of the 29 patients (
Fig 5).
In addition, foraminal widening was observed in one (14%) of the seven
volunteers and in five (17%) of the 29 patients.
Dimpling of the annulus capsule due to the
secondary retraction effect of the increased disk length was observed on
the sagittal
MR images obtained in three (43%) of the seven
healthy volunteers and in 12 (41%) of the 29 patients (
Fig 6) (
Table 2).
TABLE 2. Dimpling of Annulus Capsules and Changes in Facet Joints and Intervertebral Foramina during Traction
Figure 5. Sagittal T2-weighted MR images (4,000/128) of the foramen at the C6-7 cervical disk level and the facet joint at the C7-T1
cervical disk level in a patient with HCD in (a) neutral and (b) traction states. The facet joint (arrow) is widened at traction (b) compared with in the neutral state (a). The width of the foramen (arrowheads) also increased with traction.
Figure 6a. Sagittal T2-weighted MR images (4,000/128) of the cervical spine of a healthy volunteer in (a) neutral and (b) traction states. Dimpling of the annulus capsule (arrow in b) is seen at traction.
Figure 6b. Sagittal T2-weighted MR images (4,000/128) of the cervical spine of a healthy volunteer in (a) neutral and (b) traction states. Dimpling of the annulus capsule (arrow in b) is seen at traction.
Discussion
Although regression of a herniated intervertebral disk at follow-up has been reported in up to 3% of cases of herniated cervical
or lumbar disks (
6,
7),
the exact mechanism of the regression of a herniated intervertebral
disk is still not understood. The disk may be subject
to desiccation and shrinkage from loss of
hydrophilic proteoglycans, which leads to a loss of water content and,
consequently,
a decrease in disk size (
7). Reports (
8,
9)
have suggested that traction therapy can induce HCD regression.
However, the mechanism of the disappearance of the HCD at
follow-up MR imaging after traction—that is,
whether it is a reduction or a spontaneous resorption—is still unclear.
In a report (
1),
it is stated that the length of a cervical disk increases during
traction. The report only describes those changes in disk
length that were identified by measuring the
distance between the bone margins of adjacent vertebral bodies on
radiographs,
however. Therefore, the reduction of a herniated
disk particle during traction could not be precisely evaluated in that
study.
If cervical spinal MR imaging could be
performed simultaneously with traction, the changes in intervertebral
disks could be
directly evaluated. A cervical traction device for
MR imaging should be made of nonmagnetic materials. In addition, the
volume
of the device should be small enough to fit easily
on the limited space of an MR gantry and coil while inducing an adequate
traction force. Therefore, we designed a device
that can be expanded by means of air inflation. With expansion of the
device,
elongation of the neck between the shoulder and the
occiput can be achieved. The device has a traction effect on the
cervical
vertebral column that is similar to that of
conventional traction methods that are applied at bedside. We used 30
pounds of
traction force (ie, pressure to the internal space
of 0.4 kgf/cm
2) because early separation of the posterior vertebral segment is induced by applying a minimum pressure of 25 pounds (
10).
In our evaluation of the changes in HCDs
during traction at MR imaging, we observed a reduced herniated nucleus
pulposus particle
through the tract of a torn annulus (
Fig 4).
This suggests that direct reduction effects on HCDs can be verified at
MR imaging performed during traction.
Although long-term
follow-up was not performed in this study, we
believe that reduction of the herniated nucleus pulposus might lead to
healing
of the torn annulus and resolution of the disk
herniation. Complete resolution or partial reduction of a disk
herniation was
seen in 21 patients; these results suggest that
traction has an effect on HCDs.
All seven healthy volunteers and 21 (72%) of the 29 patients with HCD showed substantial elongation of the cervical vertebral
column after the traction device was applied and inflated.
In a cadaveric study (
11),
there were significant increases in the intervertebral foraminal volume
and the size of the area at the foraminal isthmus.
We also induced a flexion posture of the cervical
spine during traction. However, neither widening of the facet joint
space
(in two [29%] volunteers and five [17%] patients)
nor widening of the intervertebral foramen (in one [14%] volunteer and
five
[17%] patients) was frequent. These results might
have been due to the thickness of sections on sagittal images, which may
have been such that very rapid changes in the facet
joint and intervertebral foramen could not be sufficiently evaluated.
Dimpling of the annulus capsule of the
cervical disk was seen in three (43%) of the seven volunteers and in 12
(57%) of the
21 patients who had elongation of the cervical
vertebral column during traction. This dimpling might have been a
secondary
effect of cervical vertebral column traction and
may represent a response to the traction. Responding to the traction,
intervertebral
disks can show dimpling of the annulus capsule by
increasing the length of disk space, which instantly results in negative
pressure on the disk. Owing to its flexibility, the
disk decreases in width to resolve this phenomenon. However, a disk
that
does not respond to the traction might not show
dimpling of the annulus capsule.
In conclusion, cervical spinal MR imaging performed during cervical traction with a portable intermittent traction device
can be used to evaluate the reducibility of cervical disk herniation with traction.
Acknowledgments
The authors thank Yong-Jae Lee, MD, for advice and support and for serving as a photographic model in the volunteer study.
Footnotes
-
Abbreviation: HCD = herniated cervical disk
-
Author contributions: Guarantor of
integrity of entire study, T.S.C.; study concepts, T.S.C.; study design,
T.S.C., C.J.P.;
literature research, T.S.C., S.W.K.; clinical
studies, T.S.C., Y.J.L., S.W.K., C.J.P.; experimental studies, T.S.C.,
C.J.P.,
Y.W.S.; data acquisition, T.S.C., W.S.K.;
data analysis/interpretation, Y.W.S., T.S.C., Y.J.L.; statistical
analysis, W.S.K.;
manuscript preparation, T.S.C., Y.J.L.;
manuscript definition of intellectual content, Y.J.L.; manuscript
editing, Y.W.S.,
T.S.C., Y.J.L.; manuscript revision/review,
T.S.C., Y.J.L., W.S.K.; manuscript final version approval, T.S.C.
Magnetic resonance (MR), functional imaging, 316.12144
Spine, intervertebral disks
Spine, MR, 316.121411, 316.121412, 316.12144
References
- ↵
Wong AMK, Leong CP, Chen CM. The traction angle and cervical intervertebral separation. Spine 1992; 18:136-138.
- ↵
Saunders HD. Use of spinal traction in the treatment of neck and back conditions. Clin Orthop 1983; 179:31-38.
- ↵
Rendina APM, Benazzo F, Castelli C, Paparella F. The statics of cervical traction. J Spinal Disord 1994; 7:337-343.
- ↵
Valtonen EJ, Moller K, Wiljasalo M. Comparative radiographic study of the effect of intermittent and continuous traction on elongation of cervical spine. Ann Med Intern Finn 1968; 57:143-146.
- ↵
Bozzao A, Galluci M, Masciocchi C, Aprile I, Barile A, Passariello R. Lumbar disk herniation: MR imaging assessment of natural history in patients with treated without surgery. Radiology 1992; 185:135-141.
- ↵
Teplick JG, Haskin ME. Spontaneous regression of herniated nucleus pulposus. AJNR Am J Neuroradiol 1985; 6:331-335.
- ↵
BenEliyahu DJ. Magnetic resonance imaging and clinical follow-up: study of 27 patients receiving chiropractic care for cervical and lumbar
disc herniation. J Manipulative Physiol Ther 1996; 19:597-606.
- ↵
Kinnaird RH, Jelsma R. A portable traction device for cervical fractures. J Neurosurg 1992; 76:544-545.
- ↵
Saal JS, Saal JA, Yurth EF. Nonoperative management of herniated cervical intervertebral disc with radiculopathy. Spine 1996; 21:1877-1883.
- ↵
Judovich BD. Herniated cervical disc: a new form of traction therapy. Am J Surg 1952; 84:646-656.
- ↵
Humphreys SC, Chase J, Patwardhan A, Shuster J, Lomasney L, Hodges SD. Flexion and traction effect on C5-C6 foraminal space. Arch Phys Med Rehabil 1998; 79:1105-1109.